Dr Pravin Badhe
Overview
AI is shifting predictive healthcare from static risk scores to continuously learning systems that anticipate events, personalise interventions, and optimise operations across the care continuum. Research interest has surged dramatically, with publication volume on AI-driven healthcare prediction increased sharply in 2025, driven by the COVID pandemic, growing availability of large-scale electronic health records (EHRs), edge computing, and real-time patient data.
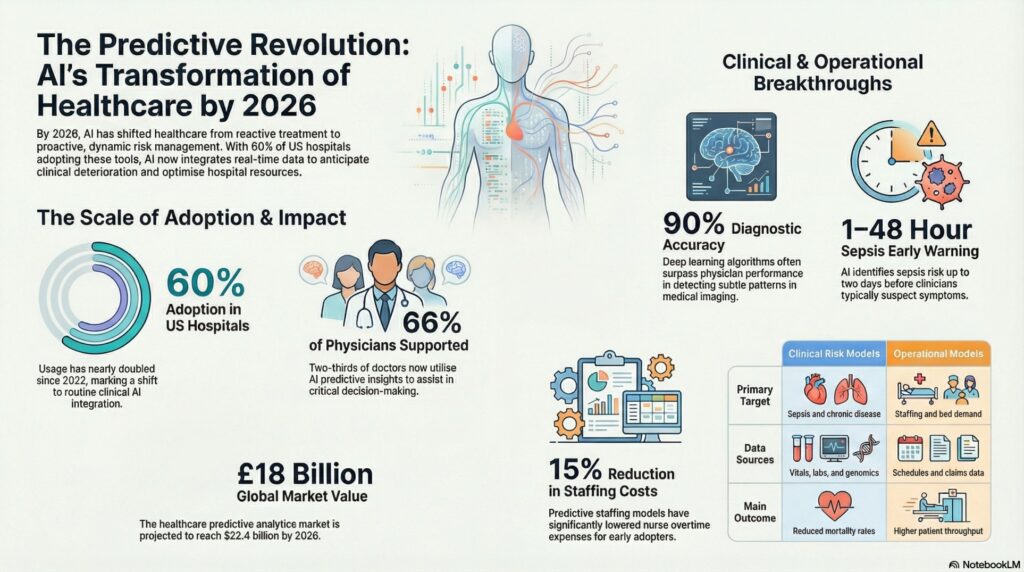
By 2026, nearly 60% of hospitals in the United States will have adopted at least one AI-assisted predictive tool in routine clinical care, up from approximately 35% in 2022. The global healthcare predictive analytics market is expected to reach $22.4 billion by 2026.
The Scale of the Shift
AI and machine learning significantly enhance predictive analytics in healthcare, enabling timely and accurate predictions that lead to proactive interventions, personalized treatment plans, and ultimately improved patient care. As healthcare systems increasingly adopt data-driven approaches, the integration of AI and data analysis has garnered substantial interest.
Key adoption milestones include:
- By 2026, ~60% of US hospitals have adopted at least one AI-assisted predictive tool in routine clinical care (up from ~35% in 2022).
- By 2026, 75% of new drug discoveries are projected to involve AI-powered predictive modeling at some stage of the R&D process.
- AI-driven predictive staffing systems have reduced nurse overtime expenses by an average of 15% in early-adopting health systems.
- Early-warning models for sepsis can flag risk 1–48 hours before clinical suspicion, improving odds of timely treatment and lowering mortality.
Core AI Techniques Being Used
The field has moved well beyond simple regression. Modern predictive healthcare models leverage a spectrum of sophisticated approaches:
Machine Learning Ensembles
The most frequently used approaches are tree-based ensemble models such as Random Forest, XGBoost, and LightGBM for structured clinical data, and deep learning architectures like CNNs and LSTMs for imaging and time-series tasks. These learn complex, non-linear relationships across EHR data, labs, imaging, genomics, and wearables.
Real-Time & Continuous Risk Scoring
Rather than producing one-off predictions at admission or diagnosis, modern systems enable continuous updating of models as new data streams are used to create dynamic risk trajectories. This enables real-time risk scoring for deterioration, sepsis, acute kidney injury, readmissions, and no-shows, often hours to days before clinicians would normally suspect problems.
Natural Language Processing (NLP)
NLP models mine unstructured clinical notes to enrich feature sets and power note summarization, risk extraction, and guideline-concordant recommendations, turning previously inaccessible free-text data into actionable signals.
Federated Learning
Advanced federated learning frameworks allow models to be trained across institutions without centralising protected health information (PHI), enabling more robust, generalisable models while preserving privacy.
What’s Changing in Clinical Care
Early Disease Detection
AI demonstrates diagnostic accuracy between 76% and 90% for imaging and clinical scenarios, often surpassing physician performance on mammograms and skin lesion detection. Deep learning algorithms detect subtle patterns in X-rays, MRIs, and CT scans that human eyes may overlook, especially under fatigue. AI risk models also stratify populations to identify individuals likely to develop diabetes, hypertension, CVD, and other chronic conditions using history, genetics, and lifestyle data enabling earlier preventive interventions.
Preventing Readmissions & ER Returns
Hospitals are using predictive models to flag patients at risk of readmission before discharge even happens. Instead of waiting for a patient to return to the ER, the system can trigger follow-ups, medication checks, or remote monitoring shifting care from reactive to proactive.
Real-Time Clinical Insight
By harnessing predictive technologies, clinicians can access integrated insights drawn from blood and urine tests, medical history, and lifestyle data all in real time. These advanced models detect patterns that humans may miss, enabling physicians to shift from reactive treatments to proactive care. AI now supports roughly 66% of physicians in decision-making processes.
Integration into Clinical Workflows
Predictive models are being integrated directly into clinical workflows via Clinical Decision Support (CDS) modules in major EHRs including sepsis prediction, deterioration indices, and ‘best care choices’ treatment guidance. Success depends on designing for humans first, creating tools that reflect actual care environments and specific pressures on nurses and physicians.
Personalization, Digital Twins & Generative AI
Multimodal ML models now combine EHR data, omics, imaging, and wearables to recommend treatments more likely to work for a specific patient and adjust chronic disease regimens continuously as new data arrives.
Generative AI and large language models are being adapted into ‘digital twin’ frameworks that forecast longitudinal patient trajectories (e.g., labs, functional status, clinical events) and simulate alternative therapeutic scenarios and their uncertainties. Digital-twin LLMs retain conversational interfaces, allowing clinicians to query why a trajectory is predicted, which variables matter most, and how different treatment choices might change outcomes.
By 2026, generative AI will be utilised in drug discovery, medical imaging enhancement, and personalised medicine, helping researchers develop new drugs faster by predicting molecular structures and drug interactions and even generating synthetic medical data to train AI models while protecting patient privacy.
Operational & Administrative Prediction
AI’s impact extends well beyond the bedside. Health systems are deploying predictive models for:
- ED arrivals, admissions, and patient flow optimizing bed management, staffing, and OR scheduling to reduce bottlenecks and wait times.
- Readmissions, falls, and care-management needs supporting targeted interventions and more efficient use of high-cost resources.
- Disease outbreaks and demand surges improving resource allocation across beds, ICU capacity, staffing, and supply chains.
- Revenue cycle and claims flagging likely denials and over-utilization, indirectly improving clinical resource availability.
Clinical vs. Operational Models: A Comparison
| Dimension | Clinical Risk Models | Operational Models |
| Primary Target | Deterioration, sepsis, chronic disease progression | Bed demand, staffing, readmissions, no-shows |
| Data Sources | Vitals, labs, EHR notes, genomics, wearables | Schedules, historical volumes, length-of-stay, claims |
| Main Outcome | Earlier intervention, reduced mortality | Higher throughput, lower cost, less crowding |
Technical & Ethical Challenges
Despite rapid progress, key challenges persist:
- Data privacy and security: Integration of patient data across EHRs, labs, and wearables raises significant privacy concerns and regulatory compliance requirements (HIPAA, GDPR).
- Model interpretability: A significant limitation of many deep learning models is that they are not interpretable, restricting clinical utility and undermining trust. Many existing approaches provide only generic post-hoc explanations rather than patient-specific reasoning.
- Algorithmic bias: Models trained on historical data can inherit and perpetuate biases from incomplete or unrepresentative datasets.
- Real-world adoption gap: Many models show strong retrospective performance but limited real-world adoption due to poor integration into clinical workflows and alert fatigue.
- Data quality: Disconnected systems leave patient data scattered across EHRs, labs, and wearables if AI cannot access clean, unified data, predictive analytics becomes ‘predictive fiction.’
Emerging best practices emphasize explainability, calibration, prospective validation, and tight integration into clinician workflows. Techniques like SHAP (Shapley Additive Explanations) are being developed to bridge the gap between model output and clinical trust.
Looking Ahead: 2026 and Beyond
The conversation is shifting from AI’s potential to its measurable impact. Healthcare leaders now recognize that technology alone will not solve their problems it must be paired with depth of domain expertise. Key trends shaping the near future include:
- A shift toward smaller, domain-specific models that balance efficiency with precision, replacing today’s bulky, general-purpose LLMs that require costly fine-tuning for healthcare.
- AI copilots for documentation and triage scaling broadly, followed by more sophisticated sequencing models combining predictive capabilities with summarization tools to make care faster and safer.
- Mature data governance programs that allow healthcare systems to automate securely and at scale, with compliance built into data pipelines.
- Greater collaboration between small innovators and larger pharmaceutical organizations rather than heavy acquisition cycles.
Ultimately, success will not be measured by how much AI is deployed, but by how well it strengthens trust, enhances presence at the bedside, reduces cognitive burden, and supports measurable outcomes like safety, throughput, and recovery time. AI in healthcare is not the future it is the present, and organizations that treat it as core infrastructure rather than an experiment will lead the next era of medicine.